Postural Orthostatic Tachycardia Syndrome (POTS) is a complex and often misunderstood condition that affects the autonomic nervous system—the system responsible for regulating essential functions like heart rate, breathing, and digestion. When this system doesn’t work as it should, it can lead to a wide range of symptoms that may appear unrelated, making diagnosis challenging.
Sometimes POTS is referred to as dysautonomia, which is an umbrella term for multiple conditions that affect the autonomic nervous system (ANS).
The ANS is like your body’s autopilot. It runs all the things you don’t have to think about—like breathing, digesting food, keeping your heart beating, regulating your temperature and sweating, balancing hormone levels, and even managing your bladder. It takes care of the body’s automatic functions so you can focus on everything else.
The ANS has two key branches that work together to keep everything running smoothly:
When these two systems are balanced, your body stays in harmony. But when that balance is off—like in POTS—it can cause a wide range of symptoms that affect everyday life.
POTS can affect anyone, but it most often appears in teenagers and young adults—typically between the ages of 15 and 50. It can also occur in children and older adults, though that’s less common.
Like many inflammatory and autoimmune conditions, POTS affects significantly more women than men. In fact, research suggests that females are around five times more likely to be diagnosed with POTS. Scientists are still working to understand exactly why this difference exists, but hormones, immune function, and genetic factors may all play a role.
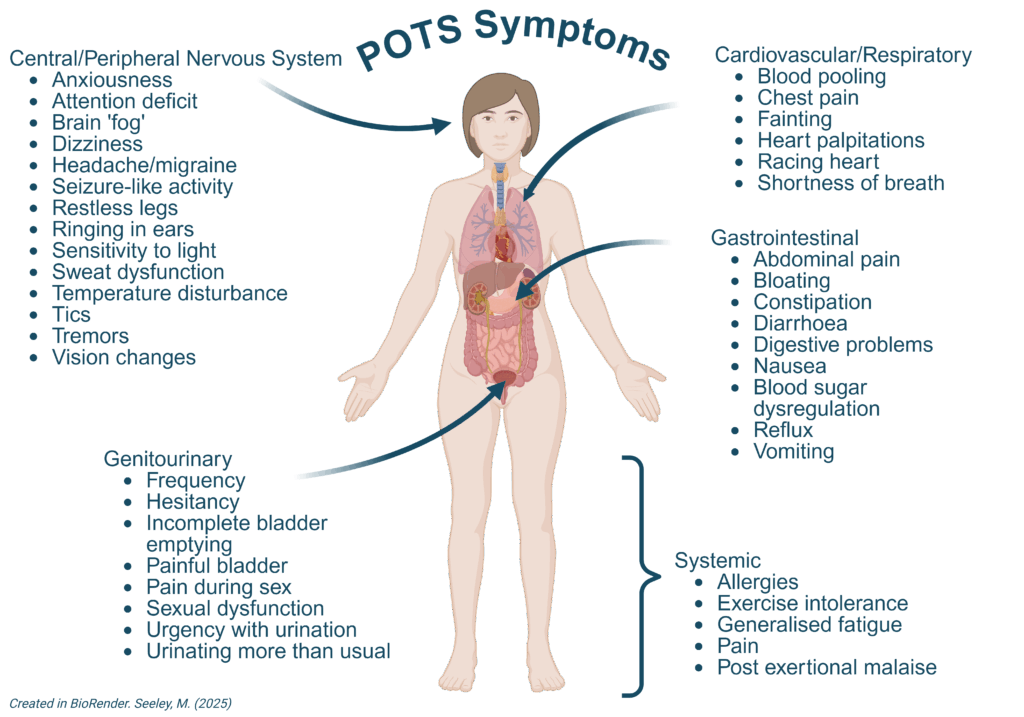
It’s important to know that POTS can affect people in various ways, and symptoms can be very different from one person to another. Some people with POTS might only have mild symptoms that they can manage easily, while others might have more serious symptoms that make everyday life harder. Symptoms might also come and go over time. POTS can bring about symptoms that affect different parts of the body including:
A key symptom of POTS is a fast heartbeat when standing up, called tachycardia. People may feel palpitations, chest pain, or dizziness due to changes in blood flow and the heart rate response to this. They may find it particularly difficult to stand for any period of time. Especially when the weather is warm.
Many people with POTS report feeling dizzy, having trouble concentrating which is sometime referred to as ‘brain fog’. Headaches, including migraines, are also common in POTS. Some people also have sensory problems like tingling or numbness.
POTS can affect digestion, causing symptoms such as feeling sick, tummy pain, bloating, or irregular bowel movements. These symptoms can make it hard to eat well and stay healthy.
Feeling tired all the time is a common feature of POTS. Tiredness might get worse when standing or doing activities because the body is working harder to keep blood flowing properly.
POTS can interfere with how the body controls temperature, making people feel too hot or too cold or have fluctuating temperature changes.
Some individuals with POTS may experience bladder problems, such as increased frequency or urgency to urinate. While others may notice difficulty emptying their bladder fully.
POTS can sometimes affect eyesight, causing blurry vision or difficulty focusing eyes. In some cases people may notice their eyes are sensitive to bright lights.
POTS can lead to sweating problems, including excessive sweating or difficulty sweating when needed.
POTS is a condition with complex origins, and its exact causes are not always clear. Sometimes symptoms start suddenly after certain events or conditions:
POTS may develop following an infection or viral illness, such as COVID-19 or glandular fever. It’s thought that the body’s immune response to the infection may trigger changes in the autonomic nervous system, leading to the onset of POTS symptoms.
POTS can also be triggered by surgery or traumatic events, including concussions. These events can disrupt the communication between the brain and the autonomic nervous system.
Hormonal fluctuations during significant life events such as pregnancy, menopause, or puberty can sometimes trigger POTS symptoms. Changes in hormone levels can affect blood volume, circulation, and the functioning of the autonomic nervous and immune system, potentially leading to the onset of POTS.
Individuals with hypermobile Ehlers-Danlos syndrome (hEDS), a connective tissue disorder, are at an increased risk of developing POTS.
Sometimes known as the ‘NASA Lean Test’ or the “poor man’s tilt”, this simple test helps doctors check for POTS. Your heart rate and blood pressure are measured while lying down, then again after standing. If your heart rate increases by 30 beats or more within 10 minutes—and you feel dizzy, light-headed, or unwell—it may suggest POTS.
To understand more about how an Active Stand Test is conducted please see the “How to Undertake and Interpret an Active Stand Test” information sheet.
If the Active Stand Test doesn’t clearly confirm a POTS diagnosis, your doctor may refer you for a tilt table test. In this specialised assessment, you lie on a motorised table that tilts you upright while your heart rate and blood pressure are continuously monitored. Although it can provide helpful insights, a tilt table test is not essential for diagnosing POTS.
Diagnostic Criteria:
To diagnose POTS, doctors look for a few key signs during testing:
To understand more about Tilt Table Testing please see the “Tilt Table Test” information sheet.
The Malmo POTS Survey is a simple questionnaire developed by researchers in Sweden to help screen for POTS. It gives doctors a better understanding of your symptom patterns and can support the diagnostic process.
You can fill it out at home and bring the results to your GP or specialist to guide further discussion.
You’ll find links to both the Malmo POTS Survey and the Active Standing Test in the resources below.
To help rule out other conditions and support a POTS diagnosis, your doctor might suggest the following:
These tests can be useful in checking for other causes of symptoms, but they are not necessary to diagnose POTS.
While there’s no cure for POTS, there are some treatments which can help to manage symptoms and improve quality of life.
Managing POTS starts with lifestyle changes, which are often the most important part of care. These strategies can help stabilise symptoms and improve daily functioning:
Boosting fluid and salt intake helps expand blood volume and improve circulation.
These are specially designed garments—such as tights, stockings, or shorts—that apply gentle pressure to the legs and lower abdomen to support blood flow.
Medical-grade compression garments are classified by their pressure level, usually starting from 15–20 mmHg for mild compression. For POTS, a pressure rating of 20 mmHg or higher is generally recommended, ideally with coverage from ankle to waist. However, any amount of compression is generally better than nothing.
While traditional medical-grade options are available through pharmacies or medical suppliers, there are now a number of brands producing functional, comfortable compression wear designed for daily use—often used by athletes or people with chronic conditions.
Members of the Australian POTS Foundation can access discounts on quality compression garments. Visit our Membership Page for details.
Staying active with POTS can be challenging, but keeping your muscles strong is important. When muscles contract, especially in your legs, they help push blood back up to your heart, which can reduce symptoms like light-headedness, fatigue, and brain fog.
Many people with POTS spend a lot of time lying down to manage symptoms, especially before diagnosis. Over time, this can lead to deconditioning, which may make symptoms worse.
The goal isn’t to push through with intense workouts, but to build a gentle, personalised movement plan that focuses on:
Many people start with seated or lying-down movements like gentle stretching, resistance exercises using bands or light weights, or recumbent cycling. It’s best to work with a physiotherapist or exercise physiologist who understands POTS or chronic illness. They can help you move safely, avoid overexertion, and guide you using tools like heart rate monitors or biofeedback.
Any movement plan should work alongside your daily life—not add extra strain. The focus is on steady, sustainable progress that supports your wellbeing.
If lifestyle changes alone do not improve your symptoms, then your doctor may consider some medications. In Australia, all medications for POTS are used ‘off-script’ meaning they are not subsidised by the Pharmaceutical Benefits Scheme.
The following medications are sometimes used by doctors to support people in managing POTS.
Midodrine: This medication helps constrict blood vessels in the legs and abdomen, helping to improve blood flow to the heart and brain.
Ivabradine: Ivabradine is another medication that can lower heart rate and improve symptoms of POTS.
Fludrocortisone: Fludrocortisone helps increase blood volume by promoting salt and fluid retention in the body.
Propranolol: Propranolol is a beta-blocker that can help control heart rate and reduce symptoms like palpitations and tachycardia.
Other Medications: In some cases, other medications such as antihistamines for allergic reactions or medications for gastrointestinal symptoms may be prescribed to help manage specific symptoms associated with POTS.
Some health and wellbeing practices have been shown to support overall physical and mental health, and may be helpful for some people living with chronic conditions.
One area of interest is vagus nerve stimulation, as the vagus nerve helps regulate heart rate, digestion, and blood pressure. Techniques that may gently stimulate the vagus nerve include:
While these approaches are considered complementary, and not treatments for POTS, some people find them helpful as part of their broader wellbeing plan.
As always, speak with your healthcare team before starting new therapies—especially if you’re unsure how your body may respond.
More research is needed to fully understand POTS and how it affects people over time. Current understanding suggests that it is often a chronic and fluctuating condition. However, with the right support and management, many people experience improvement in their symptoms and quality of life. Many are able to return to study or work, build families, and enjoy activities that bring them happiness and meaning. Everyone’s journey is different, but there is hope, and you are not alone.
POTS can significantly impact a person’s ability to attend school or work regularly. Symptoms like dizziness, fatigue, brain fog, and pain can lead to frequent absences and make it difficult to concentrate or keep up with daily demands.
For students, it’s important that families work with the school to develop an Individual Learning Plan (ILP) or other flexible arrangements. These may include modified timetables, rest breaks, or exam accommodations. For more information, see our POTS in Schools, TAFE and University resource.
For adults, flexible work arrangements—such as reduced hours, remote work, or adjusted tasks—can help support your capacity to stay engaged at work. You’re encouraged to speak with your employer about adjustments that may help, such as:
To assist with these conversations, we’ve developed a Workplace Adjustments resource.
For more information on other organisations that provide supportive services please visit our Resources Page.
A POTS diagnosis can feel overwhelming, but you’re not alone. By becoming a member of the Australian POTS Foundation, you’ll gain access to support, practical resources, and discounts on essentials like compression wear and hydration products. For a small annual fee, you’ll also join a growing community advocating for better care nationwide. Learn more on our Membership Page.



